Several other factors are compounding the shortage:
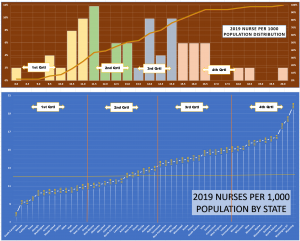
- Location: estimates of nursing shortages at the state level are all over the place, with some states projected to have large shortages (CA >200K by 2030) and some avoiding it all together (“if” the current ratios of RNs per 1,000 population hold!)
- Rural communities: absorb greater impacts of the nursing shortage than do metropolitan areas. About 1 out of every 6 RNs live in rural areas, where they serve over 50M Americans.
- Lack of faculty: nurses need to be taught by other nurses. But faculty is also retiring leaving nursing schools without a strong pipeline of educators to take their place. The 2020 AACN survey discovered that over 80K qualified applicants to nursing schools were turned away due to a lack of qualified faculty, classroom space and budget constraints. As a result, fewer nursing graduates will be joining the workforce.
- Job morale: heightened stress levels of today’s nurses are due to more than just the pandemic, more than just the need to make urgent life-altering decisions, and more than just working long hours. It’s all of these things and more, combined, that weigh on the shoulders of many RNs.
- Misguided budget plans: based on calculations of care hours (HPPD) have led many healthcare facilities to cut staffing levels or delay recruitment, leaving a major imbalance in the workloads for remaining nursing staff.
- The pandemic: created the need to move nurses from their typical care roles to the critical care covid units and to furlough others from traditional procedural areas. Both contributing to increases in nursing retirement.
- Some are leaving for greener pastures: to the private (pharma, biotech, etc.) and advance practice clinical sectors. The average nurse practitioner earns well over $100K, while the average nursing school assistant professor earns $75K